Our Vasectomy Reversal Results
We publish our real outcomes, including complications, and update them periodically as follow-up results come in. The figures below cover our 2025–2026 results.
Does It Work Even Years After a Vasectomy?
Often, yes. In our series to date, success rates have stayed high well beyond the 10-year mark, including our longest interval of 25 years. The evidence suggests the chance of success declines gradually with time rather than falling off a cliff, and our experience so far is consistent with that.
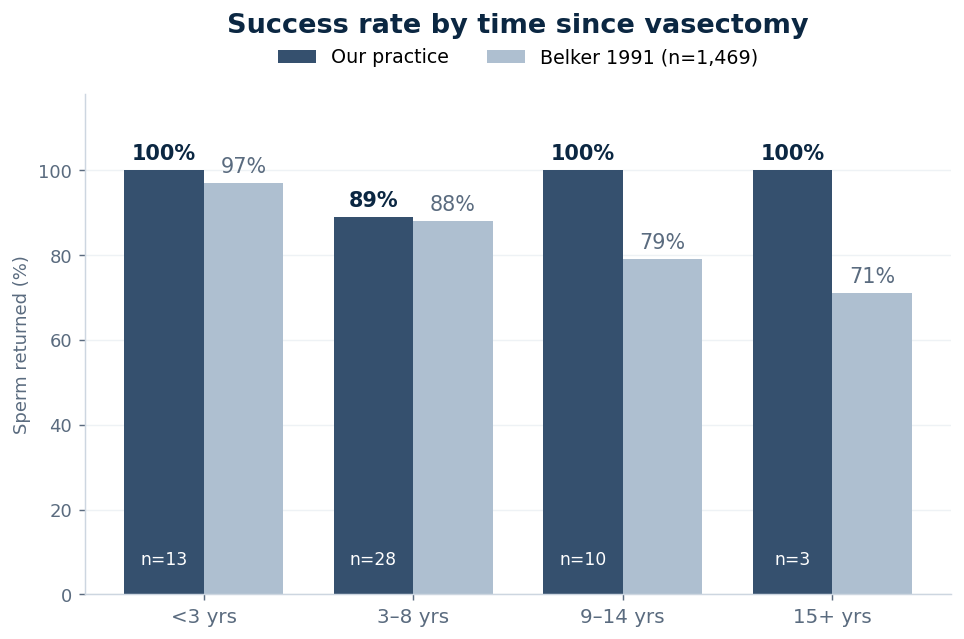
A note on reading this chart: the later time bands are based on small numbers of patients so far (10 men at 9 to 14 years and only 3 beyond 15 years), so those percentages will move as more results come in. A single patient makes a big difference when the group is small. The published series (Belker 1991) includes 1,469 men, which is why it is a steadier guide to what to expect over the long term.
Who We Treat
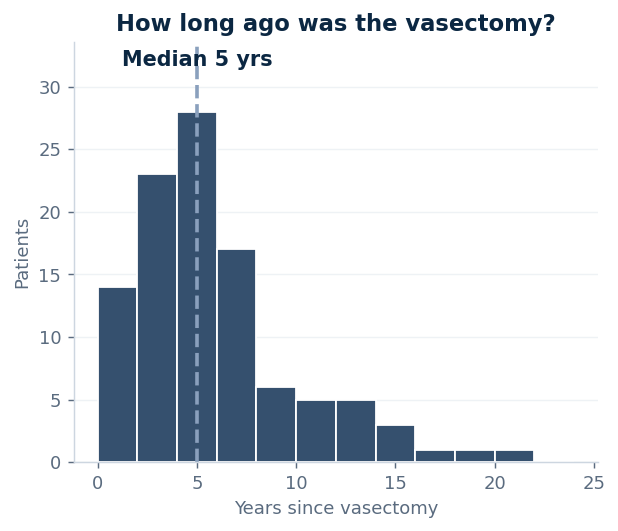
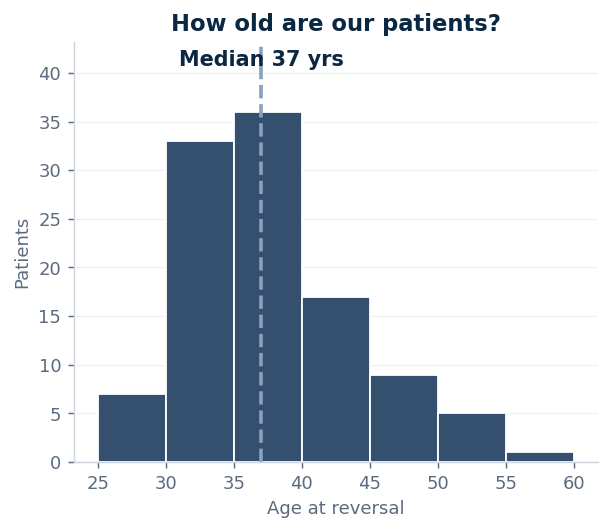
Our patients range from their late 20s to age 60, with a median age of 37. The typical patient is about 5 years out from his vasectomy, though nearly a quarter are 8 or more years out.
How Our Results Compare With Published Series
The largest meta-analysis of microsurgical vasovasostomy, covering 31 studies and 6,633 patients, reported an overall patency rate of 89.4% and a pregnancy rate of 73.0% (Herrel et al., 2015). The landmark multicentre series by the Vasovasostomy Study Group reported patency of 97% under 3 years, 88% at 3–8 years, 79% at 9–14 years, and 71% beyond 15 years (Belker et al., 1991). Our figures sit in line with these published results, although our series is smaller and our follow-up is shorter. We report them here so that patients can see real, current numbers from the practice they are considering rather than relying on quoted literature alone.
Time since vasectomy remains the most important predictor of success, and partner factors matter as much as surgical ones for eventual pregnancy. As both the published data and our own series suggest, a long interval alone does not rule out a good outcome.
How We Measure Success, and What These Numbers Mean
Success is confirmed by a laboratory semen analysis showing the return of sperm ("patency"). Of the patients who have completed post-operative testing so far, 94% had sperm return and the majority had counts in the normal range. Several pregnancies have already been reported. Patency is not the same as pregnancy: conception also depends on factors including partner fertility and time.
The first semen analysis is usually done around 2 to 3 months after surgery, so our most recent patients have not yet reached their first test. As in any surgical practice, not every patient completes follow-up testing, so these figures reflect those with results available and will be updated as more come in. In one case an initial reversal did not restore sperm and a second procedure achieved patency; that patient is counted once, by his final result. Individual results vary, and no outcome can be guaranteed.
Complications
We record every complication using the Clavien-Dindo classification, the standard system for grading surgical complications, and report them all here, including minor ones. Across all operations to date, our rate of a hematoma (a collection of blood under the skin) requiring any intervention has been under 1%. Minor, self-limiting hematomas that settle on their own without treatment are a recognised event after any scrotal surgery. We have recorded no other complications requiring intervention.
A small number of repairs can also narrow or close again over time: we have recorded one confirmed late failure and one patient with a declining sperm count on follow-up. The late-failure patient passed his initial semen analysis and so is included in the figure above; late closure is one reason we continue follow-up. We mention these because honest outcome reporting includes the results that are less favourable, not only the successes.
Separately, and not a complication: roughly 2% of planned procedures are stopped at exploration when the findings suggest a reconnection is unlikely to succeed. That is a decision made together during surgery, and in that situation patients pay only the $2,000 exploration fee, as set out on our pricing page.
Figures reflect outcomes recorded as of 6 July 2026. Success rates are reported against the number of patients with a completed post-operative semen analysis, with denominators shown in the charts. References: Belker AM et al. J Urol 1991;145(3):505–511. Herrel LA et al. Urology 2015;85(4):819–825. This information is provided for general education and is not a substitute for an individual medical consultation.
Have Questions About Your Own Chances?
Your initial consultation with Dr. Lombaard is free and by telephone. We will talk through the factors that apply to your situation.
Book a Free Consultation